Empowering Science Education
teachers & scientists working together to enhance school science
Join us in building strong partnerships that empower teachers with the latest scientific knowledge and resources, ensuring that students continue to view science as an engaging and practical subject.
The Teacher Scientist Network (TSN) is a Norfolk-based science education charity that has for 30 years provided links to ‘real science’ and supported science teachers in a truly bottom-up way. We continue to do this from our home at the John Innes Centre providing
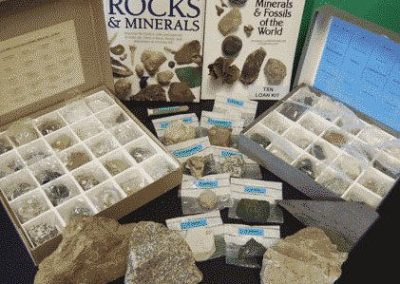
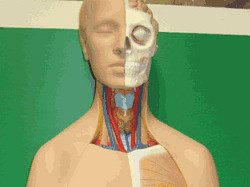
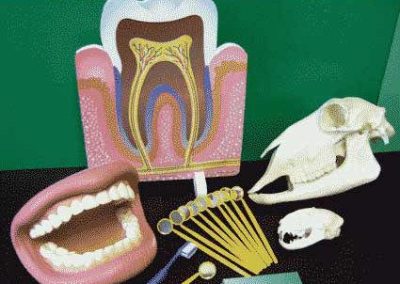
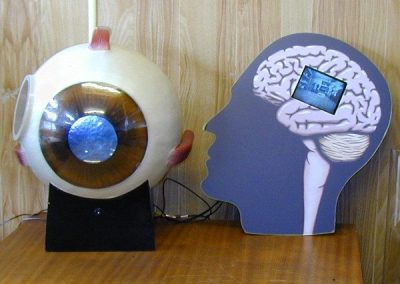
- Access to science resources via our Kit Club
- CPD opportunities to boost your subject knowledge
- A sense of community and opportunities for Networking with colleagues
- Opportunities to support scientists wishing to engage more schools, providing training and working collaboratively on the development of new resources for schools
Latest News and Events
A successful Norfolk Science Teaching Conference
Almost 50 teachers joined us at the 2nd Norfolk Science Teaching Conference doubling the attendance from last year. The event has a real buzz about…

Kits heading East
This year has seen the start of a productive arrangement with Kingfisher Schools Trust who are based in Leiston, Suffolk. Every half-term, a…

Biotechnology training sessions – dates announced
Would it be easier for you to access kit in Cambridge, Kent or Hull – see details of other summer CPD. Teacher and technician training will…

Norfolk Science Teaching Conference 2026
Join the Teacher Scientist Network at this unique conference for both primary and secondary school teachers, with hands-on workshops, free…

Portable Planetarium training event
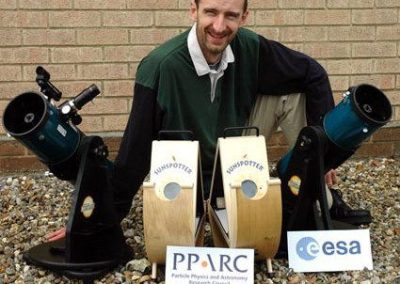
Participants from 5 new schools joined us recently (in the squash court!!) to learn everything about loaning the Portable Planetarium. This…

MEGAWATT
MEGAWATT – Free workshops and resources on energy and sustainability. TSN is delighted to make you aware of a FREE opportunity for KS3/4 science and…
Our Kit Club


























What Our Participants Say
“Our school will be continuing with the subscription as they are such a valuable resource.”
Sarah
Wensum Junior School
“Collaborating with scientists through this network has enriched my classroom experience and inspired my students.”
David Brown
“The resources and support provided by the Teacher Science Network are invaluable to any science educator.”